Obstruted Defaecation Web
| ODS Secondary to Abnormal Uterine Descent |
|
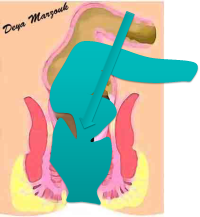
This is a rare cause, but may actually be the major cause of ODS in some younger patients. On straining the uterus moves significantly backwards, pressing on the anterior rectal wall to actually block rectal lumen. This is best appreciated, using digital rectal examination whilst asking the patient to bear down. The following flash animation illustrates this [Click to start].
A distinction can be made between 2 groups. First, it is occasionally found in combination with other anatomical abnormalities in ladies aged 30s & 40s who have had several children or had long standing defaecatory symptoms & have been straining for years. These patients are usually severely symptomatic & may have associated perineal descent or type 3 internal rectal intussusception or may have even just developed external prolapse. They almost always need surgical intervention. Second and much more rarely, it can be seen as an isolated cause in much younger ladies, as young as 16-18 years of age. These tend to be much less symptomatic [possibly because it is isolated and bad defaecatory habits such as straining hard, have not been firmly established] and they tend to respond to education & conservative management. Management is the same as other patients. Conservative management is offered first, except in patients with type 3 internal rectal intussusception, who should be offered surgery to start with. Rectal irrigation techniques is distinctly unpopular in these younger ladies & those who fail conservative measures would proceed to surgery. Because many of patients in this group did not have pelvic surgery [e.g. hysterectomy] and have not yet developed significant diverticular disease, it may be possible to consider laparoscopy & Trans-STARR or traction Trans-STARR [REPLACE] as an option, although laparoscopic resection-rectopexy, with deep pelvic dissection and cul-de-plasty is generally a better option as it often leads to better postoperative function compared with the laparoscopy & Trans-STARR option. All patients who undergo surgery MUST have uterine suspension as well. |